
by Dr Nagnath Khadke
Rheumatoid arthritis (RA) is the most common chronic inflammatory arthritis. It is characterized by pain, swelling and stiffness in multiple small and large joints of upper and lower limbs.It can lead to joint destruction and deformities leading to physical disability and significantly affects quality of life.
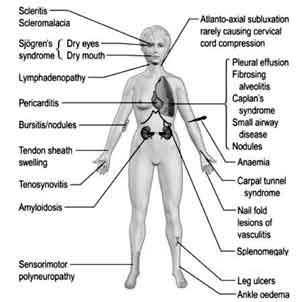
Although primarily RA affects joints, because of the systemic nature of the disease, it can affect number of different organ systems in the body. These are labeled as extra-articular manifestations.They may develop before or after the onset of arthritis and can be seen in about 50 % of cases at some point of disease.
Patients with Early(Young) onset, positive blood tests for RA (RF & ACCP) & smoking are most likely to develop extra-articular disease.
These may involve any organ system including important organ systems like Lungs, Kidney, blood etc.Subcutaneous nodules, secondary Sjögren’s syndrome (dryness of mouth), pulmonary nodules, and anemia are among the most frequently observed extra-articular manifestations.
The extra-articular manifestations can be asymptomatic to severe and sometimes even potentially fatal. Some manifestations are minor like Rheumatoid nodules which do not require any special treatment. Some are severe like Interstitial lung disease, which can cause significant disability and require specific treatment, while some can be potentially fatal like pericarditis (inflammation of the coverings of heart), vasculitis (inflammation of the blood vessels) which need to be dealt urgently and aggressively.
However most of these manifestations gives us some warnings or clues beforehand.If these warning signs are recognized early, rheumatologist can manage these easily without resulting in significant harm to the patient. Hence there is requirement of closely supervised and monitored treatment in case of RA.
| Neurological | Peripheral neuropathies Entrapment Neuropathies(carpal tunnel syndrome) Mononeurits multiplex Myelopathy Stroke Atlanto-Axial subluxation |
| Ocular | Xeropthalmia (dry eyes) Sclerits/Episcleritis |
| Cutaneous | Rheumatoid nodules Peripheral vasculitis Leg ulcers Alopecia |
| Haematologicall | Haematological Anaemia Neutrophillia Thrombocytosis Felty’s syndrome |
| Pulmonary | Pleural effusions Interstitial lung disease Bronchiolitis oblitrans Pulonary nidular disease Pulmonary arterial hyper tension |
| Cardiac | Pericarditis Coronary vasculitis(rare) |
| Others | Dry mouth Osteoporosis Muscle wasting Atherosclerosis Renal involvement |
| RED FLAGS | Atlanto-Occipital subluxation Pericarditis Scleritis Peripheral vasculitis Monoarticular flare |
- NEUROLOGICAL MANIFESTATIONS
In RA all parts of nervous system can be affected, including Brain, Spinal cord and Peripheral nerves.
NEUROPATHY - Neuropathy (affection of nerves) is not uncommon in RA. Most common is peripheral neuropathy &mononeuritis multiplex (affection of multiple different nerves at a time). Perception of tingling & numbness or burning sensation in hands and feet, slipping of footwear unknowingly, difficulty in lifting the leg off the ground are commonly observed symptoms. Early treatment is essential in good recovery, hence these symptoms should be reported to rheumatologist at the earliest.
CNS DISEASE
- Brain matter affection is not very common. Patients can have stroke (blockage in supply of the blood to a part of the brain) most commonly resulting in different symptoms depending upon the part of the brain affected.
These symptoms can range from tingling numbness, imbalance, tremors, and paralysis of a part of a body to loss of consciousness, coma or death in severe cases.
MYELOPATHY
- Spinal cord affection is in the form of myelopathy, due to various causative factors.Myelopathy can give rise to temporary or permanent paralysis like Quaduplegia (paralysis of all the four limbs), paraplegia (paralysis of both lower limbs), loss of sensation in limbs or trunk, difficulty in walking or loss of bowel bladder control and many other symptoms.
Many of these manifestations can be picked early on thorough examination and managed. Hence the need for continuous follow up in RA.
ATLANTO-AXIAL SUBLUXATION
One of the most important manifestation is atlanto-axial joint (2nd joint of vertebral column) involvement, which may be clinically asymptomatic until the subluxation develops. Development of pain at the back of head, radiating arm pain, numbness or weakness of the limbs and giddiness on neck movement are warning signs; if not picked up this can be sometimes fatal on inadvertent neck manipulation.
It can be picked up by imaging (Xray) of cervical spine (neck).Surgical correction can be done if required.
OPHTHALMIC (EYE) MANIFESTATIONS
Eye manifestations are very common in RA.These include Sjogren’ssyndrome , keratitis, scleritis, episcleritis, corneal ulcers, secondary cataract and various other less common disorders.
Sjogren’s syndrome is characterized by dry eyes & mouth. Patients usually complain of a sandy or gritty feeling in eyes. Other symptoms include burning, decreased tearing, redness, itching, eye fatigue, and increased photosensitivity.
These symptoms are due to destruction of eye lining and glands producing tears. If treated early it does not result in any visual disturbance.It can be easily evaluated and diagnosed by a very simple test called as Schirmer’s I test.
All of these eye complaints if treated early do not lead to any significant visual disturbance/loss, but if ignored can lead to significant vision loss and disability.ence one should not ignore these eye symptoms as minor and report it to your specialist (Rheumatologist) for early diagnosis and treatment.
Nodules
Firm, non tender subcutaneous nodules seen in 30–40% of patients. It is one of the diagnostic criterion of RA.
Nodules are found most often on extensor surfaces or pressure points,such as on the elbows, Achilles tendons, and fingers.May also occur in the lungs, pleura, pericardium, and peritoneum.
Nodules are typically benign, although they can be associated with infection, ulceration, and gangrene.Cutaneos nodules require no specific treatment, while pulmonary nodules require regular follow up to detect changes in the size or shape of nodules.
In case of pulmonary nodules other possibilities require exclusion. Complications arisingfrom the nodules (eg, hemoptysis (blood in sputum), pneumothorax (air trapping in coverings of lungs) should be treated directly.
Other cutaneous manifestations are –
Palmar erythema (redness at the finger extremities and on palms),
Palpable purpura (tiny red eruptions over skin),
Livedo reticularis (lacy, dusky purple, asymptomatic discoloration seen on the extremities),
changes of vasculitis (blackening of nail folds, blackening of finger extremities with severe pain),
Pyoderma Gangerenousum (ulcerative skin disease most commonly in the form of rapidly progressing, painful ulcer).
Anemia (reduction in haemoglobin levels), Neutropenia (reduction in white blood cells) and thrombocytosis (increase in number of platelets) are common haematological manifestations in RA
Anemia
Anemia is the most common hematologic abnormality in patients with RA.Causes of anemia in RA patients are numerous & include Nutritional deficiency (iron / vit b 12 / Folate deficiency ), GI loss (loss through stoamch , deoudenal ulcers), Ineffective erythropoisis (i.e improper utilization of iron and other nuitritional molecules by the body ) and drug induced.
Anemia causes easy fatigability, generalized weakness and many other symptoms leading to poor quality of life. Anemia is also a risk factor for heart failure in patients with heart disease for which RA patients are prone. Hence it should be not neglected.
Regular follow ups and blood checks helps us in identifying it early. Anemia can be easily treated with simple medicines and dietary measures.
Neutropenia
Neutropenia , Thrombocytosis are other known extra articular hematological manifestations.
Neutropenia means reduction in number of white blood cells, which are an important part of protective forces of our body.It can predispose the patient to various common, uncommon and hospital acquired infections.Hospital acquired infections are difficult to treat as many of the organisms causing them are now resistant to routine antibiotics.
As many RA patients are exposed to immunosupressive drugs, neutropenia becomes a major health hazard in such patients.Also we can effectively monitor it through routine simple blood tests. If recognized early and managed properly we can avert major complications.
Thrombocytosis
Thrombocytosis (increase in number of platelets) is a generally an asymptomatic condition and needs treatment only when symptomatic.
There are at least six forms of lung disease in RA, as follows:
Pleural disease (affection of lung coverings)
Interstitial lung disease (affection of lung substance)
Nodular lung disease (formation of nodules in lungs)
organizing pneumonia
pulmonary hypertension (increase in the pressure inside blood vessels supplying lungs )
Small airways disease (asthma like disease)
These shows that pulmonary manifestations can occur involving any part of the lung, including blood vessels, parenchyma (lung substance), and pleura (lung coverings).
Lung involvement can occur due to various other causative factors. Drugs used to treat the disease, such as methotrexate, can cause pulmonary problems.Treatment with TNF inhibitors can lead to reactivation of pulmonary or extrapulmonary tuberculosis.
RA patients who smoke are likely to be at a higher risk for pulmonary complications than are patients in the general population.
Most common symptoms are cough & pleuritic chest pain in pleural diseases, cough & dyspnea in parenchymal diseases.Solitary or multiple Pulmonary nodules can occur in RA, and need to be differentiated from carcinoma.
These are important manifestations as they affect activities of daily living. These manifestations may remain silent for long period before producing any symptoms.
Also these need to be differentiated from the symptoms caused by other diseases.History and chest examination is essential with chest X ray and pulmonary function tests adding valuable information. HRCT and 2 D Echo are necessary for complete evaluation. Their early recognition helps in effective management and decreases the possibility of considerable morbidity otherwise. Hence the need for regular visits and time to time checkups as advised.
Treatment is disease specific. For manifestations like interstitial lung disease, new treatment in the form of biologic injection is quite effective.
Every tissue and organ of the body is dependent on uninterrupted supply of blood for its function. This supply is through the blood vessels which are responsible for maintaining vital organ function.
In vasculitis these blood vessels are affected by inflammtion. Hence it can affect any organ of the body including important organs like kidney, brain etc. It is rare but important manifestation of RA, Seen in patients with long standing disease, many times in well controlled disease.
When small arteries are affected it may cause digital infarcts, painful ulcers and gangrene, resulting in significant morbidity and functional disability.
Impairment or compromise of the blood supply to the organ leads to derangement in that particular organ function, for example in case of kidney it leads to decrease in the urine formation causing accumulation of harmful substances in the body.
Treatment should be aggressive with immunosupressives.For skin gangrene or tissue loss grafting can be done in some cases.
It has become apparent that the increased risk of premature death in RA is due largely to an increased incidence of cardiovascular disease, primarily myocardial infarction and congestive heart failure. Even in RA patients without clinically evident cardiovascular disease, cardiac dysfunction can be present.
Similar to lung involvement, cardiac manifestations can occur involving any part of the heart, including heart coverings, heart muscles, heart valves, heart chambers, conduction (electrical system) of the heart and blood vessels supplying heart.
ECG , 2D Echo, holter monitoring are some of the available tools for cardiac evaluation in such cases.
Atheroscerosis
Atherosclerosis is today the single most important risk factor for cardiac disease and cardiac disease is one of the leading cause of death/mortality.There are multiple risk factors for coronary artery disease in RA patients in addition to the risk factors that are relevant in the general population. Patients with long standing RA have more atherosclerosis than patients of the same age with more recent disease onset.
Common symptoms of cardiac disease are shortness of breath, chest pain, palpitations, easy fatigability and swelling over body. These should be reported to the specialist at the earliest.
Cardiac diseases lead to considerable morbidity and mortality, and hence need to be prevented or treated at the earliest. Management is disease specific.
kidney is rarely involved directly in RA, but often is compromised indirectly by therapy.
NSAIDs are the most common culprit in renal derangement. Amyloidosis is an unusual complication of chronic RA.Amyloidosis, along with vasculitis (blood vessel affection) and sepsis (blood infection), is one of the most important life threatening complications of RA.
Osteoporosis today is a silent epidemic. population above 60, tobacco use, post menopausal status, steroid use, chemotheorapy, renal failure are few of the common risk factors for osteoporosis.Because postmenopausal women are more at risk for RA and for osteoporosis, this group should be treated aggressively.
Minimizing steroid use is one method to decrease the risk of osteoporosis in this group and other patients with RA. Bone densitometry should be performed routinely in patients with RA, and treatment with calcium, vit D supplementation and bisphosphonates should be started.
Therefore diet of RA patients should contain fruits rich with calcium and milk which is a good source of Calcium. Early morning sunlight provides Vit D.
Few of the extra-articular manifestations are important and may lead to significant damage if not recognised& treated early.These are called as RED FLAGS.
Atlanto-Occipital subluxation
Pericarditis
Scleritis
Peripheral vasculitis
Monoarticular flare
This has been discussed in detail earlier.
Usually presents as central chest pain, cough and breathlessness.Needs urgent investigations and urgent initiation of steroid therapy.Tuberculosis should be ruled out.
Presents with sudden onset of eye pain and increased watering. If left untreated this may lead to loss of vision.
SUMMARY
Extra articular manifestations of RA are not uncommon. (seen in up to 50 % patients at some point of disease)
Sometimes these are asymptomatic requiring only observation, but sometimes can become potentially fatal.
These need to be diagnosed early in order to prevent potential major illness / functional disability.
Many of these can be missed by the patien , but picked up by your rheumatologist on examination. Hence one should have a regular follow up.
Most of these can be managed effectively and show good response to early management