
by Dr. Vinaya Kunjir
Radiologic investigations are the starting point for diagnosis and disease assessment of any joint pain. Here we are going to briefly discuss general aspects of knee joint imaging and in particular arthritis.
How is the knee joint formed
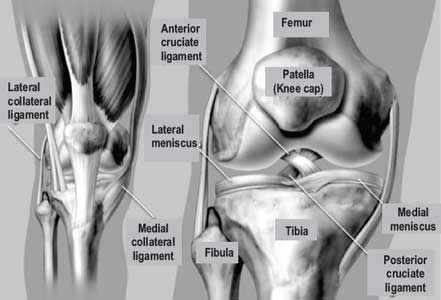
Knee joint is the complex synovial joint formed by thigh bone (femur), Tibia (bone in the leg) joined in front by smaller knee cap i.e. patella. Apart from these, smaller bone (fibula) is seen alongside tibia in the leg. The bony ends forming the joint are covered by the articular cartilages.
The bones forming the joint are supported by ligaments and menisci. These also help to regulate movement at the knee. Anterior cruciate (ACL) and posterior cruciate (PCL) ligaments as well as the medial collateral (MCL) and lateral collateral (LCL) ligaments provide stability to the joint and prevent sliding. C shaped medial and lateral menisci lie between femur and tibial articular surfaces and function as shock absorber.
Knee X RAY/ RADIOGRAPH
Common knee views taken are antero-posterior (AP), weight bearing PA, lateral (Lat) and skyline view.
The AP view is looking at knee held directly from the front. Weight bearing PA view is taken to detect early arthritis. The Lateral view is taken looking from the side perpendicular to the AP view. Skyline view is taken with knee in bent position and it assesses the joint between knee cap and femur.
Cartilage is not visible on X ray so even though the cartilage covered bone ends are in proximity to each other there appears to be a gap between them on X ray. The gap is nothing but the joint space; it is divided into medial and lateral compartments and is of uniform and even height in normal knee.
Imaging
Osteoarthritis of the knee is the most common degenerative disease affecting men and women. Knee is also a common joint to be affected in other rheumatic arthritis and acute & chronic infections
What do we see on X ray in Knee Arthritis?
Joint alignment and bone density
Joint space
Joint space reduction which can involve entire joint or selectively involve only the medial compartment. It is an early indicator of the joint degeneration and inflammation.
Degenerative changes
Though cartilage is the most affected part, it cannot be directly seen on X ray. Osteophytes (bony outgrowths), Spiking of tibial spines are the prominent features seen on radiograph.
Normal Joint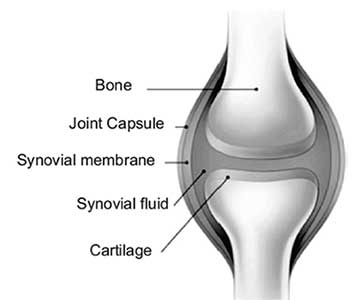 |
Osteoarthritis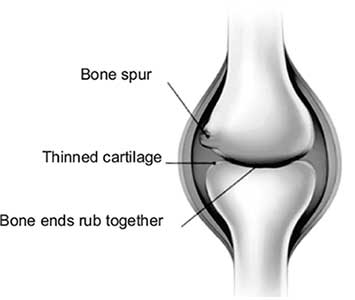 |
|
| Normal Joint |
Rheumatoid Arthritis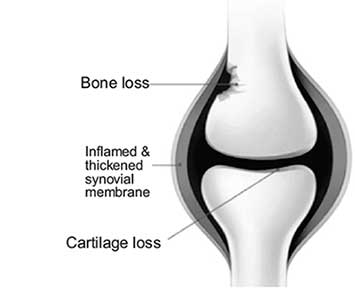 |
|
 X ray Knee AP view-OA |
 X ray Knee AP view-RA |
X ray radiography remains the most important investigation for diagnosis, assessment and monitoring of the inflammatory and degenerative joint diseases. It is cheap and easily available. Arthritis has typical imaging appearances especially in well established cases.
Soft tissue swelling commonly seen above the patella on lateral view is an indicator of either the fluid in the joint or the synovial thickening.
ULTRASONOGRAPHY (USG)
Features of arthritis take time to progress and so changes in disease status seen on plain films are relatively slow to develop. USG and MRI detect these changes early. Ultrasonography (USG) is cost effective and dynamic investigation. It shows the amount of joint fluid and soft tissues in the knee joint like synovium and cartilage. Ultrasound is a valuable diagnostic tool in assessing muscular, tendinous and ligamentous damage (chronic and acute) bursitis seen in inflammatory arthritis.
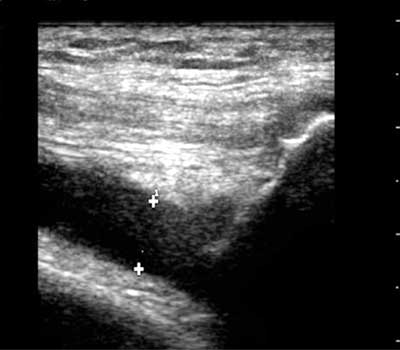
Fluid in the knee Joint
Ultrasound also provides the cost effective way to assess clinically occult disease.
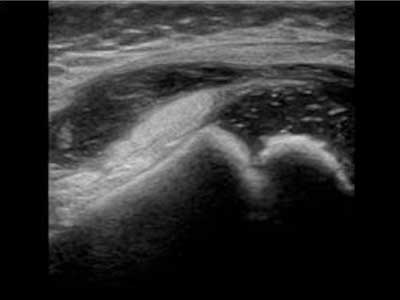
Synovial thickening and Effusion
CT and MRI
CT scan and MRI visualize the knee joint in all three dimensions. While CT is better for looking at the bone, MRI gives very good view of soft tissue structures. Both these scans detect the early disease and characterize them better.
MRI can show both joint inflammation and joint damage and accurately detect structural and inflammatory lesions of all joint structures including tendons and tendon sheaths. Synovium is the most affected in case of rheumatoid arthritis. The synovial thickening with increased vascularity is very well detected on USG as well as on CT and MRI.
CT is limited due to radiation dose while imaging time, cost and postural inabilities limit the use of MRI.

In summary X ray has an important role to play in the diagnosis of many rheumatological conditions and it will continue to be an important tool for the monitoring of disease progression and assessment of therapeutic response. However clinicians are progressively turning to USG and MRI for detecting the earliest (often subclinical) changes of arthritis and it is likely that these tools will play an increasingly important role in the diagnosis of arthritis in the future.